This post presents solid evidence of items that are statistically significant based on 226 samples of people with Autism. The intent of this post is show the guns. Getting fingerprints and other “why” detective work is not included. This is just the statistical facts… painting a narrative is for others to do.
The following bacteria association with Autism is P < 0.01 or more significant. This is using the current 218 contributed samples.
When the Frequency seen is higher than Control, then there is too many. Additionally, the average amount seen in the list below is also higher than that seen in the Control. Same logic applies to those that are lower.
The probability of significance is using Chi2. A value of 6 is about P < 0.01, higher values are even more significant. As you will quickly note: Bifidobacterium for many species is too high.
I am a high functioning autistic person (which is a major factor in microbiome prescription being created — some autism characteristics allowed me to be super focused and not bored creating it), I know part of my issues was low grade coagulation issues — not usually deemed clinical significant usually. Coagulation impacts oxygen flow to the brain… which impacts behaviors. Hypoxia (low oxygen – i.e. from being at altitude without oxygen) have the following symptoms:
Euphoria
Headache
Increased response time
Impaired judgment
Drowsiness
Confusion or foggy decision making
And also speed of acquiring learning.
I did a little searching and found most of the items were very recent publications:
“The complement and coagulation pathways may be activated in the peripheral blood of children with ASD and play a key role in the pathogenesis of ASD.”
“45 differentially expressed proteins (DEPs) were identified between the ASD group and the control group. They mainly were associated with platelet degranulation, ECM proteoglycar, complement and coagulation cascades, selenium micronutrient network, …”
“It was shown that there is a statistically significant positive correlation (R=0.369, p=0.018) between the acquired immunity parameter: the level of serum antibodies to myelin basic protein (BMP): abBMP parameter, and the main parameter of platelet hemostasis – the time of appearance of spontaneous clots (Tsp).”
“Moreover, in terms of platelet functions, the elongation in collagen-ADP and collagen-EPI closure times were significantly higher for the ASD group (P = 0.044). These results may suggest an impairment in platelet functions rather than in platelet morphology for children with ASD. Considering these results, further investigation of thrombocyte functions in the ASD may lead to a better understanding of the pathogenesis of ASD”
“It was shown for the first time that clotting (hypercoagulability) of the blood plasma in patients with autism and childhood schizophrenia was increased. “
Autism is a variety of conditions caused by DNA mutations, environmental influences and a host of other factors. A significant contributor can be the microbiome. This impact can be further amplified because many children with autism are picky eaters shifting the microbiome further. What is discussed in this post applies to this child and not autistic children in general.
Back Story
A son with autism. He had COVID in April 2021. With autism, it can be challenging to identify long COVID symptoms from autism symptoms. “We have seen marginal improvements in his receptive language and command following. His social skills and emotional understanding is poor . His diet has largely remained the same , vegetables and chicken , lamb, beef or fish and spices. He is verbal but not conversational, does not sleep well at night, does stimming throughout the day, his understanding is minimal He has very good energy levels and is playing till he sleeps on most days. He has very good memory and learn preferred topics quickly but is unable to focus on any task , he is unable to write or hold pencil for long . He cannot always reply to questions and has ecolalia[unsolicited repetition of utterances made by others] . ”
Analysis
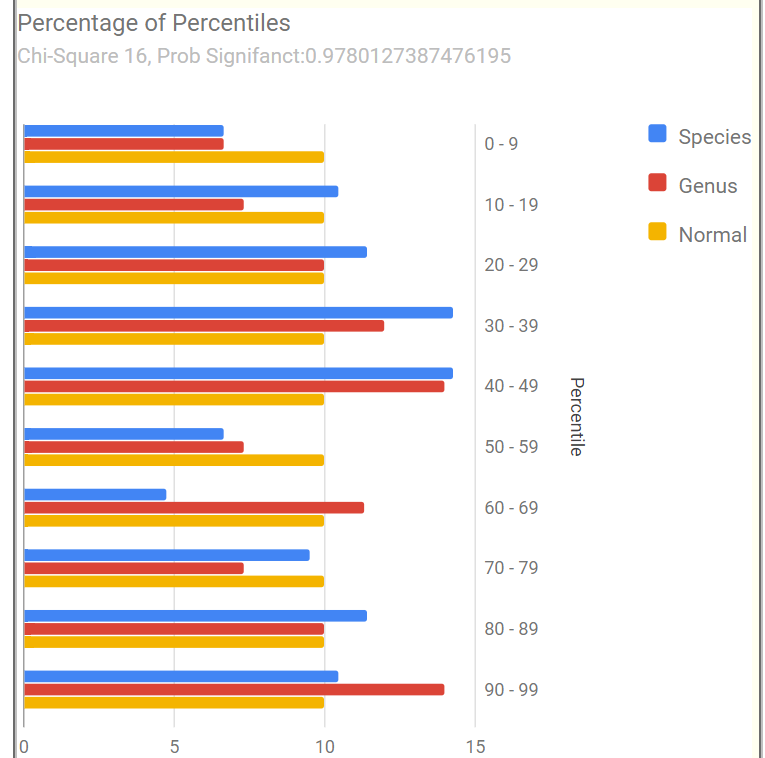
Lookin at Percentages of Percentiles, I see a different pattern than seen with ME/CFS and Long COVID — my most frequent analysis types. He has statistically (between 2 and 5%) significant abnormalities, but far less than people with ME/CFS and Long COVID.
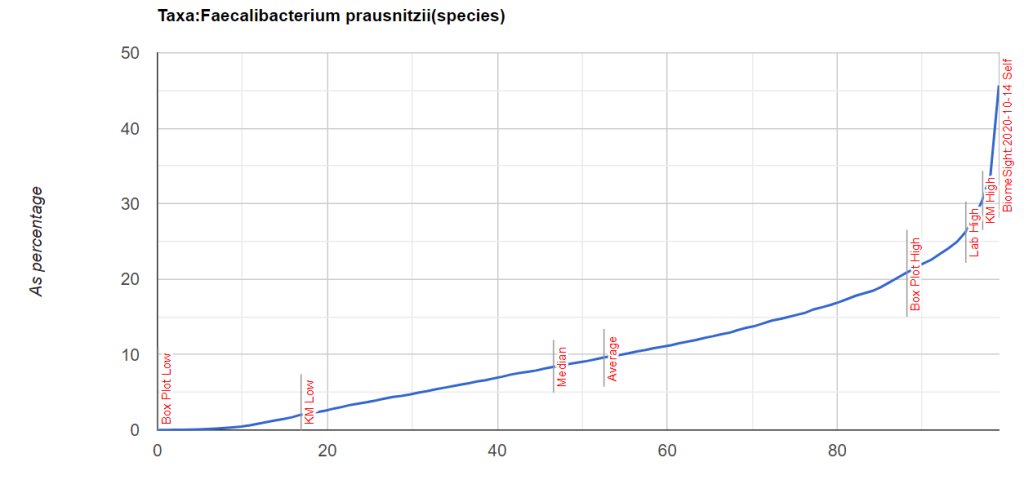
Looking at Potential Medical Conditions Detected we see that ADHD and Mood Disorders patterns are there. Everything is reasonably in range for Dr. Jason Hawrelak Recommendations with two significantly out of range (too low) is Akkermansia (which is available as a probiotic) and Faecalibacterium prausnitzii is too high (27%). This pattern is seen across all of his samples.
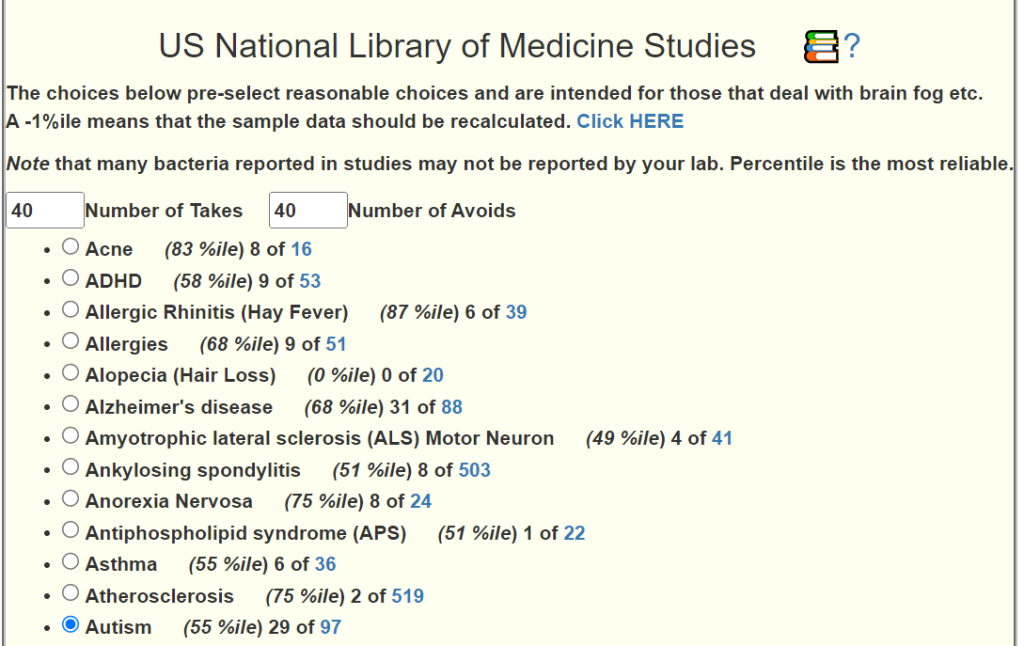
Going over to our Citizen Science Special studies, the top three pattern matches are for:
COVID19 (Long Hauler)
Autism
Brain Fog
These also are seen with an earlier sample from 2020.
Plan for Suggestions
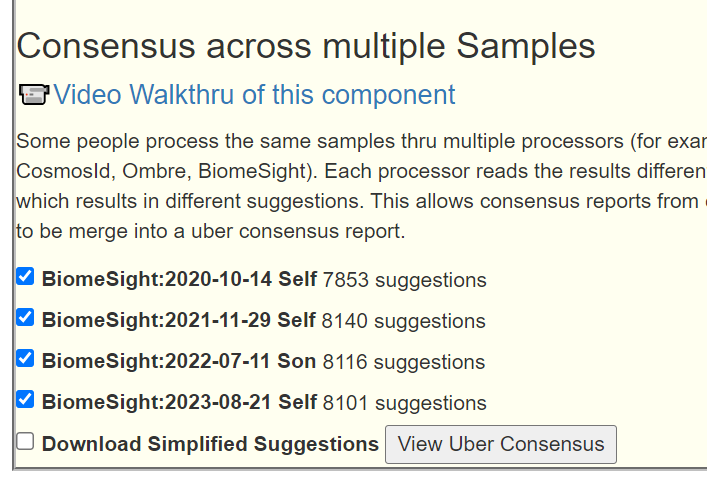
Since this is a persistent state with reasonable continuity across samples, I am going to go the Uber-Consensus route. By this I mean we will do for Each Sample:
“Just Give Me Suggestions” which executes 4 algorithms
Citizen Science using Autism
Then we combine the suggestions from each sample into one, an uber suggestion consensus. The advantage of this approach is to minimize minor fluctuations of the microbiome over time. This means that we have 20 sets of suggestions combined.
I was disappointed with the results — nothing was consistently suggested. I experimented and found that the last two samples gave more consistent results. This implies that there has been significant changes in the microbiome over the last two years.
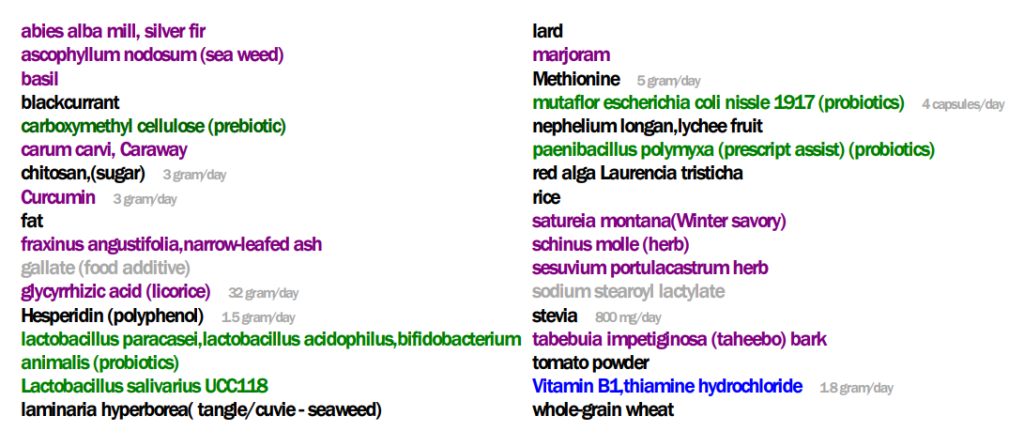
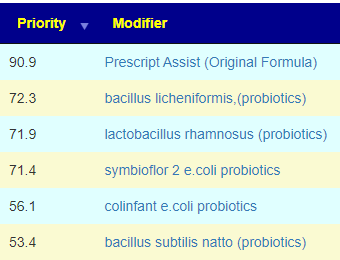
The top suggestions from the PDF are below
As a FYI, in terms of how many times things were suggested:
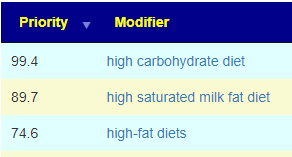
I should talk a bit about the apparent contradiction with low-fat diets vs lard and fat. These come from the terms that clinical studies used. Low fat diet tends towards fish and poultry, lard is a pork product – I speculate that the type of fat may be significant.
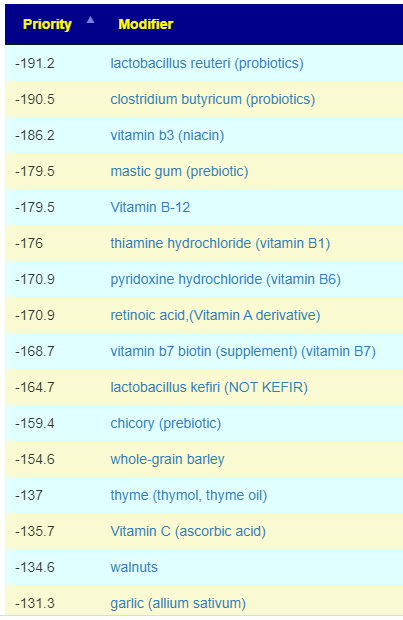
On the flip side, we have these avoids. One item seems to be to suggest gluten free (despite wheat being a to-take):
As an experiment/learning activity — I looked at some of the suggested prescription items and checked if any are used for autism. We are matching these items impact on the microbiome and the shifts that this person has (autism as a diagnosis was not considered).
Since the non-prescription items above should cause similar shifts (and likely with less risk of side effects), it appears that the algorithms are making reasonable suggestions.
The process of checking suggestions derived exclusively from the microbiome against clinical studies for a condition is called cross-validation. When there is a high percentage of agreement, it implies that the mechanism may be via the microbiome and generating candidate substance from the microbiome may produce good results.
KEGG Based Suggestions
These use data from Kyoto Encyclopedia of Genes and Genomes to try to identify substances that the microbiome and the body may be short of which can be obtain via supplements or probiotics.
Probiotics (in decreasing priority)
Escherichia coli – which can be Mutaflor (recommended above) or Symbioflor-2 (which is easier for people in the US to get).
There were several items that are counter-indicated from the suggestions – when there is disagreement, don’t gamble — ignore
Akkermansia muciniphila – low positive score but also identify as low on Dr. Jason Hawrelak Recommendations
Supplements (again double checking across suggestions and keeping only that both agree with)
Q: His gut according to the test is in good condition. I have heard in the past from one of his doctors that his Gut results were one of the best that he has seen in Autistic children, but we have not been able to make a considerable shift in his symptoms in the last few years.
A: My working hypothesis is simple: symptoms are associated to microbiome shifts. He has bacteria shifts that are matches to autism drugs (see above); so I believe further improvement of the gut and behaviors are possible and probable. He may be good; I believe he can be better.
Q: Faecalibacterium prausnitzii is high in my son , I have read it works as anti-inflammatory , but on the contrary I have heard that children with ASD have an inflamed Brian ,I would have thought this would have worked in his favor.
A: Excellent question! Faecalibacterium prausnitzii is anti-inflammatory for Crohn’s disease[2008], colitis [2013]. I was unable to find any clear literature on its effect on the brain. I did found some information that cause me to suspect that it does not impact the brain significantly.
“A 15kDa protein with anti-inflammatory properties is produced by F. prausnitzii, a commensal bacterium involved in CD pathogenesis. This protein is able to inhibit the NF-κB pathway in intestinal epithelial cells and to prevent colitis in an animal model.” [2017] – the size of this is very important.
“Most proteins in the plasma are not able to cross the blood—brain barrier because of their size and hydrophilicity.” [Basic Neurochemistry]
“does not have a barrier against molecules less than 1 kDa.. may form a barrier against molecules larger than 4 kDa” [2020]
Bottom Line — it appears the chemical produced by Faecalibacterium prausnitzii may be too big to reach the brain.
We also find the following reported, suggesting we want to reduce it to a normal range, you should independently research this
“Faecalibacterium predicted social deficit scores in children with ASD” [2018]
“Faecalibacterium prausnitzii … were also found to be highly correlated with Autism Treatment Evaluation Checklist (a measure of Autism severity )”
On the flip side, it reduces abdominal pain and improved bowel movement in ASD [2018].
“Gut microbiome data revealed Akkermansia sp. and Faecalibacterium prausnitzii to be statistically lower in abundance in autistic children than their neurotypical peers with a five and two-fold decrease” [2021] — which may account for the gut issues.
“Compared with healthy controls, Faecalibacterium,..were more abundant in ASD patients” [2021]
Your son’s range is thus very atypical being many, many times higher than expected.
I have caution here, Faecalibacterium and cognitive issues have inconsistent reports [2021, 2023 ], Faecalibacterium is implicated in cognitive issues[2018]. IMHO, encouraging it to the normal ranges may be the wisest course.
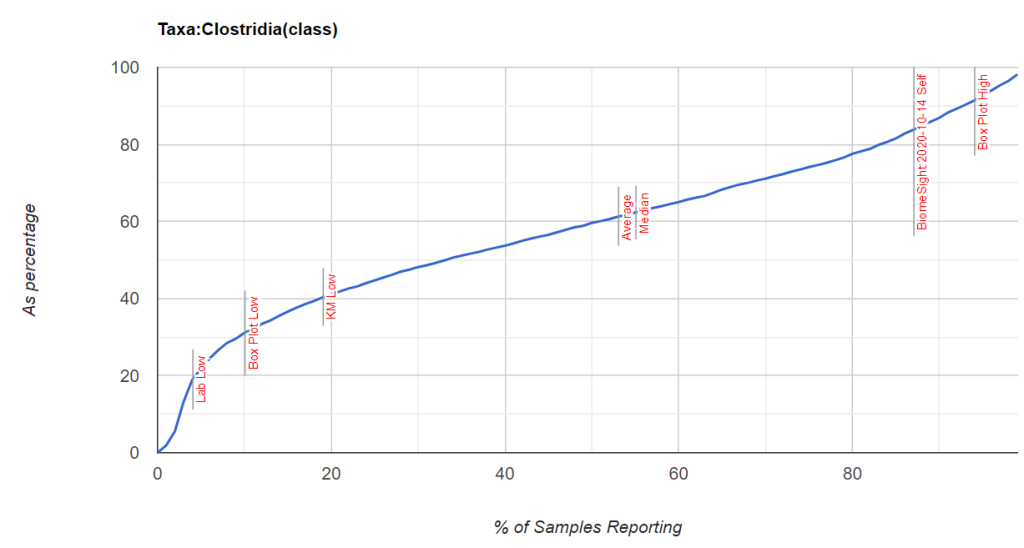
Q: “His results are over all satisfactory ,same as last year about – Gut wellness score – 89.52. I have noticed that Clostridia is about 79.7 % could this be the reason, would appreciate your help.”
A: Clostridia has been high in most samples, I drilled down into it’s main components
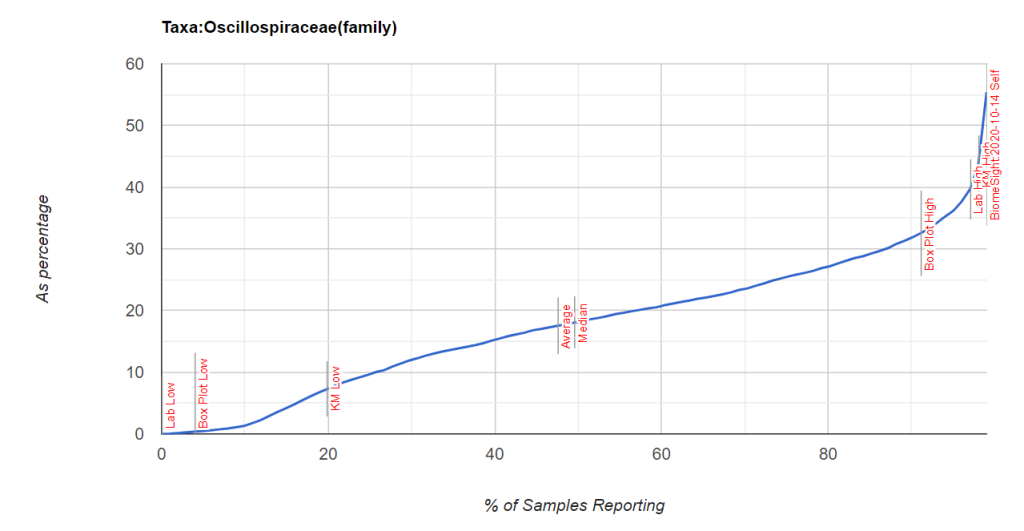
Searching for Faecalibacterium + autism on PubMed resulted in 29+ studies. There was nothing found for Oscillospiraceae + autism. Looking at the latest sample, only 10% of the organisms in Oscillospiraceae could be identified in the sample — no smoking gun for which genus. Doing a Metagenomic Shotgun Sequencingtest would like provide more information (for example, Thorne) — but it is unlikely that will produce more actionable item — just give names.
Looking at what reduces Oscillospiraceae, we see Bumetanide, cycloserine, cefixime and chlorpromazine in that list (as well as many of the above suggestions).
Some visuals: Clostridia is not that extreme, but two of it’s children are.
Microbiome Prescription uses over a million rules to generate suggestions on improving the microbiome and hopefully reduce or moderate autism behavior. All of the sources of the rules are studies on the US National Library of Medicine. Microbiome Prescription also can provide the complete evidence trail for every suggestion! That is, where — precisely– is all of the information coming from — none of it is private personal opinion or speculation.
Cross Validation
Cross validation is the process of taking one set of information to generate forecasts or suggestions and then look at a totally independent source of information to see if the forecasts and suggestions are valid, reasonable, and appear to help individuals with the condition. I have done that for several conditions with very good results. NOTE: Everything is generated by code — code that I prefer to improve or correct. I have no personal stake in the suggestion, nothing to defend.
The process is simple: some items may have been tests in trials for autism, some have not. If it has been tried, we see what the result in and provide a link to the study (open data!! no “trust me, I am an expert” hype)
“Binding studies show that both the B. subtilis and human ASLs bind up to 4 mol of APBADP per mole of enzyme tetramer and that both enzymes exhibit cooperativity: negative for B. subtilis ASL and positive for human ASL.” [2008]
Randomized controlled trial of sulforaphane and metabolite discovery in children with Autism Spectrum Disorder [2021] “Sulforaphane (SF), an isothiocyanate from broccoli, is a multifunctional phytochemical that has several demonstrated benefits on cellular processes relevant to ASD, including cytoprotective, antioxidant and anti-inflammatory responses, mitochondrial and synaptic function, neuroinflammation and neuroprotective mechanisms, as previously reviewed”
One item that is complex/questionable – depends on the child’s DNA
The goal / objective of Microbiome Prescription is to make suggestions that are more likely to help than to hurt. That goal seems to be accompanied. A secondary goal is to suggest items that have not been studied but modelling suggests that it may be of benefit to try. We have 5 such items above.
Remember these are GENERIC Suggestions for GENERIC Autism
The results of an individuals microbiome will be different — there are many variants and subsets for Autism. Each variant will tend towards their own set of variations for the microbiome. Using an individual’s microbiome sample will get suggestions unique for them.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Kang and colleagues created a modified FMT procedure called MTT for autistic youngsters [29]. This therapy alleviated ASD behavioral symptoms to some extent, with excellent tolerance indicated and improvements lasting 2 years after treatment ceased….Fascinatingly, microbial metabolic genes for folate biosynthesis, oxidative stress defense, and sulfur metabolism were dissimilar from those found in normally developing (TD) patients at ASD baseline but mirrored those found in TD and/or donors following MTT [56].
Several investigations in recent years have indicated qualitative and quantitative changes in the gut flora in a variety of neuropsychiatric illnesses, supporting the role of Gut Microbiome (GM) in the maintenance of physiological condition in the CNS. Within neurobehavioral disorders, it appears that at least a portion of ASD instances are linked to, and maybe reliant on, the health and wellbeing of the GM.
Caution: FMT can be tricky — determine the appropriate FMT sample to use is still being investigated. The donor microbiome should exhibits none of the shifts documented below, ideally the opposite direction.
Based on the literature cited here. We find the most frequently reported listed below. Note that Lactobacillus is high 8 times and low 5 times. My usual attitude when there are such contrary results is to ignore this species entirely.
This leads to the following probiotic suggestions:
Do not use Lactobacillus — it is unclear if it will help or hurt
Supplement with Veillonella probiotics when it becomes available.
Tax_Name
Direction L – Low H – High
Studies
Bifidobacterium
L
13
Lactobacillus
H
8
Coprococcus
L
7
Prevotella
L
7
Streptococcus
L
6
Veillonella
L
6
Dialister
L
6
Bacteroides
L
5
Lactobacillus
L
5
Parabacteroides
L
5
Sutterella
H
5
Clostridium
H
5
Candida
H
4
Clostridium perfringens
H
4
Collinsella
H
4
Desulfovibrio
H
4
Sarcina
H
4
Megamonas
H
4
Fusobacterium
H
4
Lachnospiraceae
L
4
Veillonellaceae
L
4
Bilophila
L
4
Blautia
L
4
Akkermansia Muciniphila
L
3
Using Microbiome Prescription
For getting a microbiome sample, it is suggested that Thorne be used because it reports Clostridium perfringens levels in almost every sample. Ombre and Biomesight only report finding it between 11–16% of the time.
Then use this to generate suggestions specific for the autism associated bacteria shifts.
Next Post — Cross Validation
Cross Validation means checking the a priori suggestions (based on above bacteria shifts) against the literature to see if they agree. Three examples are above where studies and suggestions are in agreement.
I am planning to update my knowledge of Autism by reviewing recent literature. Taking different scopes in each set.
Before birth factors
Prenatal exposure to per- and polyfluoroalkyl substances increases risk [2021]
“People are most likely exposed to these chemicals by consuming PFAS-contaminated water or food, using products made with PFAS, or breathing air containing PFAS.” [National Institute of Health]
“High maternal exposure to PFAS was consistently associated with increased abundance of Methanobrevibacter smithii in maternal stool. ” with some association to the infant microbiome. [2023]
“Valproic acid (VPA) was reported to increase the prevalence of ASD in humans as a consequence of its use during pregnancy. ” [2020] [2017]
“Maternal prenatal antifungal use and frequent prenatal antibiotic use are associated with an increased risk of ADHD in offspring” [2023] [2023] [2021] [2019]
“Children of mothers with hypertensive disorders of pregnancy (HDP) have high rates of preterm-birth (gestational age < 37 weeks) and small-for-gestational-age (SGA), both of which are risk factors of autism spectrum disorder (ASD). ” [2023]
“maternal prenatal exposure to lithium from naturally occurring drinking water sources in Denmark was associated with an increased ASD risk in the offspring.” [2023] [2023]
“We found the previously reported relationship between precipitation and autism in a county was dependent on the amount of drinking water derived from surface sources in the county.” [2012]
Comment: PFAS etc. is more likely to be present in surface sources
“women who gave birth by caesarean delivery were more likely to stop exclusive breastfeeding in the first 4 months, and those children who were not exclusively breastfed at 4 months were more likely to have autism-like behaviours “[2022]
“Children with ASD have a shorter duration of breastfeeding, a later introduction of complementary foods, and poorer acceptance of complementary foods than typical children…The research suggests that continued breastfeeding for longer than 12 months may be beneficial in reducing ASD symptoms” [2023]
“Difficulties during breastfeeding, breast milk refusal and avoidance of taking solids have been linked to ASD. Infants with ASD have been referred to as picky eaters. Problematic mealtime behaviour during infancy has also been associated with ASD.” [2022]
“Constipation in early childhood was correlated with a significantly increased risk of ASD.” [2023]
“Compared with children who did not use antibiotics during the first year of life, those who received antibiotics had a reduced risk of ASD ” [2018]
Comment: Could the antibiotics inhibit microbiome shifts contributing to autism?
As a FYI, I have taught Artificial Intelligence for Chapman University, worked as a AI/Software developer for Amazon and Microsoft. Artificial Intelligence is composed of a large number of very different techniques, at one end you have “ponies” and at the other end “Space Shuttles”. One technique, expert system with fuzzy logic (ESFL), appears to be the best. Why? Most of the techniques require vast quantity of training data and usually produce black box suggestions/predictions which lacks explanations of why. ESFL provides a complete logic/evidence trail for each suggestions/predictions which can be walked. If one piece of evidence is disputed, it can be removed easily and a new set of suggestions/predictions produced.
Build our own AI Autism Model?
This post comes from the success of using AI on Microbiome Prescription. It would be nice to see if we can do the same with Autism. The goal is to use all available knowledge from studies.
I would suggest using SWI-PROLOG as the main engine. Prolog is a language that does not compute numbers but compute logic. The following is actual program code. It is almost english-like and prolog can resolved what you should take or not take.
“take” above says get the list of items that helps and then removes all items that hurts. I.e. only items without contradictions.
The number of lines (statements) to explicitly write Microbiome Prescription in SWI-PROLOG is about 15 million statements. That code code be licensed (for free or nominal cost) to a project of this type so building such a microbiome resource is not needed; rather just augment that data with autism specific data.
One key difference between ESFL is the ability to infer and not just parrot (typical Machine Learning). Bacteria A increases IL 10. A person with SNP ABC has decreased IL 10, thus we can desired to increase Bacteria A for people with SNP ABC.
Vision – Do it For Autism!
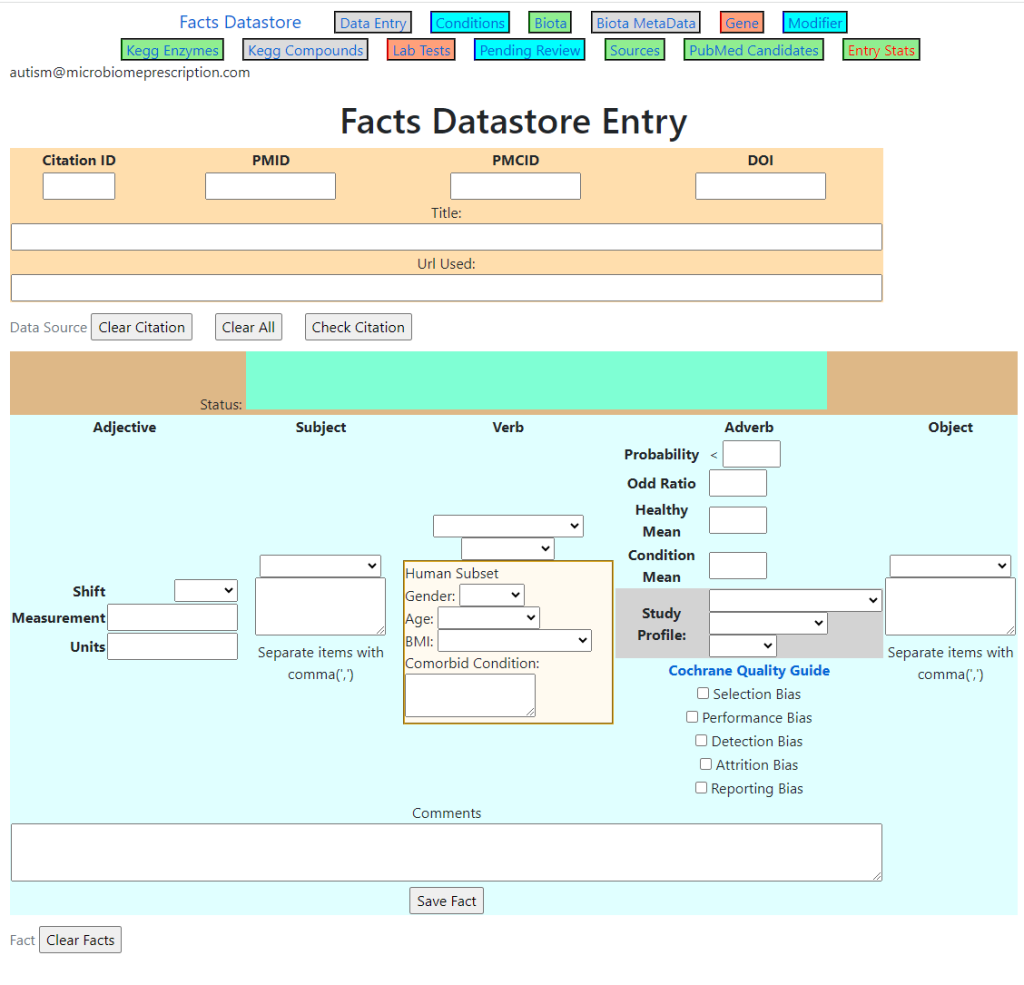
I have a web based data entry system (that is being used commercially) that can be made available to the project (with hosting of site and database). We have an almost ready to run system.
The Rub
This is a time consuming process to enter the data and then have the data reviewed (to insure correctness). Typically the people doing the entry and reviews are M.Sc., Ph.D. or M.D. Using students working on their degrees (summer work, part time) to do entry is often a way of keeping costs down. These students typically have access to the full text of articles through their educational institutes.
Typical time per study/article is 30 minutes to read and enter, 10 minutes to review
There are 72,000 studies citing Autism on the US National Library of Medicine.
A complete coverage would be 36,000 hours or 900 man-weeks or a team of 18 people working full time for a year.
The expected number of facts will likely be around 120,000.
Facts should be put in a Public Domain Type of License
This allows other groups to continue the work and prevents the need to duplicate the effort of encoding the same studies multiple times. The terms of license should require people that uses and extends it to also make their additional data available under the same terms.
Benefits
One of the key benefit is the identification of gaps in the knowledge base as well as identifying areas where there are contrary results. This allows better funding of research to fill gaps and not duplicate existing work.
A secondary benefit is that it could always be kept current and provide far more specific data for a patient based on all of the information available. The issue of MD’s knowledge being stale or bias is reduced.
What is needed — FUNDING AND MANAGEMENT
The Rub above takes money to happen — even if you are paying students the minimum wage, we quickly get a significant cost. Ideally one or more existing Autism Organizations can be persuaded to partially or fully fund this project.
My own role would be at most, a process consultant. Working Pro Bono.
Any ideas why olive oil would cause severe aggression tantrums?
From a reader
This is an interesting question.. When I see “severe aggression tantrums”, my mind goes to hypoxia (shortage of oxygen delivery to the brain).
The most significant impact of short-term memory loss for a person with hypoxia is that it impairs the ability to retain and recall new or unfamiliar information. Behavioural changes. The person may become more verbally and physically aggressive. They may also have issues with disinhibition
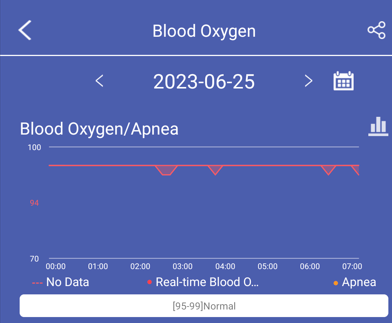
A continuous monitoring with a Saturated O2 monitor may reveal this shift (it may not, if the inflammation is in the brain — the monitor is unlikely to record it). For myself, I use a relatively cheap smart watch that records SO2 every 10-15 minutes as part of my normal proactive health monitoring, see Monitoring watch for CFS and other Conditions.
This is just a model, with some ability to check the mechanism.
My son is 5.4 years old , he was diagnosed with autism at 22 months of age .
We have been strict gluten free casein free sugar free no processed food since his diagnosis .
For almost 2 years we followed the ne chek protocol with olive oil, fish oil and 1/32 spoon of inulin.
My son was always verbal with alphabets , numbers colors , planets shapes , colors etc and the odd one / two word request sentences but never conversational.
His receptive language was very poor until maybe the last year where he is able to follow simple one step instructions.
He now repeats what is said to him and can answer to what is your name and other v simple questions .
He is not potty trained and does not understand social norms . He interacts with family members and other adults ( other adults mostly for his needs )
He eats mainly veg and chicken , fish or lamb . Occasionally rice but mostly carb free.
He consumes a lot of bananas in a day (5-6).
Foreword – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Reminder: the purpose of these posts is show the process. Every individual will get different suggestions, the suggestions should not be used viewed as suggestions for any symptom or condition.
The percentile overview shows a moderate bias toward rarer bacteria.
Percentile
Genus
Species
0 – 9
22
37
10 – 19
22
21
20 – 29
17
13
30 – 39
8
12
40 – 49
11
14
50 – 59
4
6
60 – 69
9
12
70 – 79
11
17
80 – 89
12
15
90 – 99
11
16
Potential Medical Conditions Detected has two very interesting items over 90%ile matches, namely:
Brain Trauma (99%ile)
Schizophrenia (98%ile)
For Autism he is down at the 81%ile
Other items over 90% tend to be age related, i.e. Alopecia (Hair Loss), hypertension (High Blood Pressure)
Dr. Jason Hawrelak Recommendations came in at 95.6%ile healthy, so no issue there
Since the interpretation of the microbiome data was done thru biomesight, we see that the top matches include:
Depression
Autism
Easily Irritated
Brain Fog
Neurocognitive: Attention, Memory, Focus
We have 8 significant pattern matches above and will use each to build a consensus of suggestions. A pattern match means that both of the following appear correct: microbiome pattern matches, the patients symptoms or issue are a reasonable match.
Speculation: The brain trauma and schizophrenia being a much stronger match than autism hints that this child issue may be more related to the microbiome than autism proper.
We have agreement between two very different paths of picking them (i.e. one by using the genomics of the microbiome and looking at the genomics of the probiotics; the other was using clinical studies reporting desired shifts for the bacteria that was selected). To put some specific brands (when not named above) see this list.
Many of the above are clustered, i.e. d-ribose and e.coli probiotics (one feeds the other); high saturated milk fat diet and (cottage cheese, galactose, lactose).
Diet style
The Avoids
The avoidance list is rich in “you should be taking items” suggested on the social media on the internet. In fact, they are contrary to the pattern that I typically see with ME/CFS or Long COVID. Everyone is different and it is good to do an evidence based approach for suggestions.
Questions and Answers
Readers usually get a chance to provide more information and ask questions before postings.
Q: we have been on a strict diet for our son, mainly we have not been doing GF/CF diet. Do you recommend moving to a full diet, i.e giving him milk and Gluten.
A: Milk and milk products – yes. Chocolate milk made with real Cacao is supported by the suggestions. I checked gluten items:
Gluten Free was a mild negative (-25) but checking for specific gluten foods, they were all more negative
Wheat was also a negative – 103
Oats was also a negative -32
Barley was also a negative -146
So, I would suggest keeping him gluten free
Q: (From Social Media): “I wonder what the effect is/was of 5 to 6 bananas a day”
A: In the suggestions, bananas was listed as a take in terms of the microbiome. Potassium is a factor for some autism (not all):


Recent Comments