I am a high function ASD person in the late 60’s. I am a data scientist, artificial intelligence engineer, former high school science teacher etc. Needless to say, the term autism or ASD was unknown while I was growing up. The classic delay in speech (I did not start talking until I was almost 9 y.o.) and other characteristics were ascribed to some form of brain damage. Three causes were speculated: forceps delivery, German Measles at 18 months and the medication that my mother was give to keep from miscarrying (she had 6 miscarriages before me).
Today, I know that I was high risk because my father was 44 when I was born (Parental Age at Conception and the Relationship with Severity of Autism Symptoms. 2019). My childhood was not fun, because I understood enough about my situation that I was in terror for most of it. The terror caused me to work hard and I found success in a very non-social activity: mathematics and mathematics competitions. I placed in the top 3 repeatedly in both my Province and in Canadian Mathematics Competitions. That’s enough of my story.
Purpose of this Blog
Over the last few years I have became focused (the typical uber focus of an ASD person) on the microbiome to deal with family health issues. My primary focus has been on myalgic encephalomyelitis on which I have written some 1300 posts here. Out of that, I developed an analysis site using reference site and citizen science site called Microbiome Prescription. I have also became active in a Facebook group The Gut Club: Stool Test Discussion Group. This group had resulted in contact with many mothers with autistic children. Needless to say, I have both empathy for the mother and for the children (been there myself before there was support!).
This site is very open to guest posts. I do request that they be well researched with links to source studies. I hate to be ‘anti-social’ and ignoring chat-board opinions and consensus — but what do you expect from someone with ASD? 😉
As interesting notes comes across my desktop, I will explore and attempt to write up posts on what we know today.
I will start this blog by copying across some blog posts that I have done on Autism elsewhere.
This is just presenting the tables for Autism derived from the methodology described in this technical post: Odds Ratios and the Microbiome. There are only two symptoms with sufficent data to compute odds ratios. If you us Biomesight, make sure your samples have symptoms entered!
Here are some odds ratios using BiomeSight data. Odds Low means when the reading is below the Median and Odds High above the Median (of those with this symptom). We use the symptom median to get balanced (same approximate size) categories. Using an average results in poorer results.
What is the difference between a Species and a Strain? To understand this, view Species as “dogs” and strains as specific types. Is picking a Chihuahua as a police dog a good choice, or a St. Bernard suitable for someone with disability living in a one room apartment?
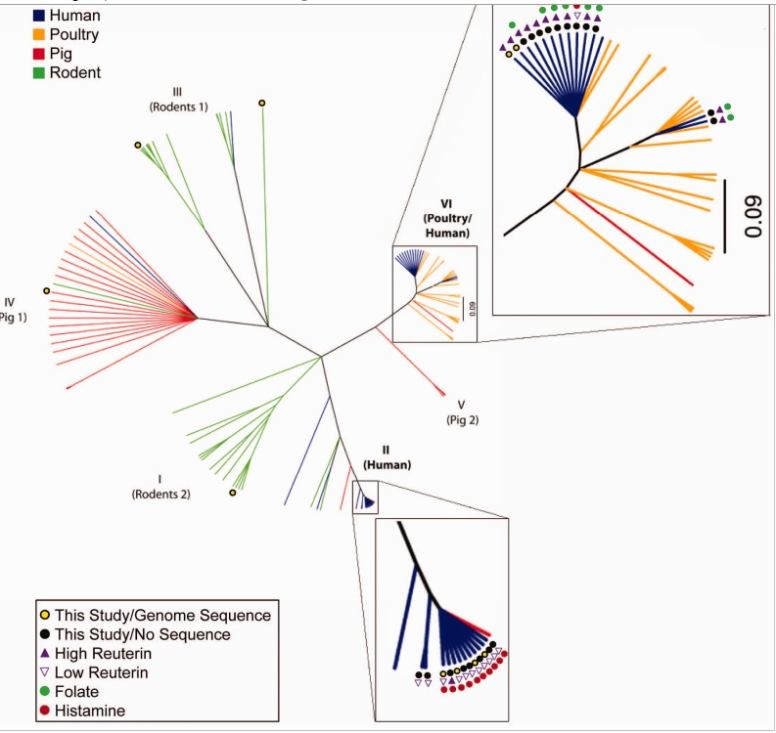
The chart below shows different aspects of different strains for Lactobacillus Reuteri. When you buy a probiotic names “Lactobacillus Reuteri”, it is unlikely which species if was obtained from is specified on the bottle. If it was not from a human, it is very unlikely that it will reproduce or take root in your body.
Probiotic manufacturers and packagers are focused on making money. They will ask for the cheapest source for a probiotic that they expect to be able to sell for the greatest profit. Human source is not a factor, cheapness is!
I have known people that are histamine sensitive that are fine with one brand of Lactobacillus Reuteri but get sick from another brand…. Looking at the chart below, the answer is obvious: One has a histamine producer and one does not.
This morning I was asked about Bacteroides fragilis BF839 which is cited in several studies on the US National Library of Medicine. Most of the studies are from 2024 or 2025. At present, it is not for sale anywhere and I do not expect it to be for five(5) years at least because of approval processes. Given the authors’ location, I expect it will be first available in China.
Researched and Stain is for sale
Several years ago I set up a free page listing those available (somewhere in the world). I also automated a weekly automatic scan of the US National Library of Medicine for any new studies using these strains. The page is kept up to date.
Occasionally, someone emails me about a new strain that has one or more studies associated. I add those to the list. If you find one that I missed, please email me!
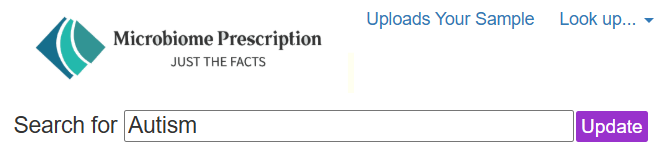
The page allows searching across the studies abstracts for key words. For example, if you are interested in Autism, just enter that and click search. The page will then show the retail brands with links to the studies.
The intent of the page is discourage random trial of probiotics which has no effect (except on bank accounts).
List of Strains with name of product or seller
At present we are at 156 different strains. These are listed below.
Akkermansia muciniphila WB-STR-0001: Pendukum Glucose Control
VSL3 / Visbiome / De Simone Formulation: Alfasigma USA, Inc.
Safest Product for Correct Identification
These strains are usually under legal protection and thus the manufacturer has a vested (financial) interest to make sure that “what is advertised is delivered”.
Why is this important, just look at some of the literature
64.4% were incorrectly labeled in either number of viable cells or bacterial species
51.6% exhibited resistance to at least one antimicrobial agent
26.8% had a lower number of viable cells than their label claims, No viable Lactobacillus was found in some products
57.8% comprised other species rather than those claimed on the contents
Your first choice should be the probiotics that are most likely to be as advertisedandhas been studied for the symptom of condition that you are interested in.
A reader requested a straightforward video on how to use the Microbiome Prescription (MP) site for her autistic child. While there isn’t an ultra-simple way, there are two main approaches:
One method is to compare your child’s results to samples from other autistic children, tested at the same lab. MP identifies which key bacteria (KB#1) to target for changes this way.
The second method uses scientific literature about autism from the US National Library of Medicine. These studies use many different labs, which are not standardized—so results can vary (KB#2).
With either method, MP suggests probiotics based on limited research. The lists of bacteria identified (KB#1 and KB#2) help determine using the novel R2 algorithm which probiotics might help, using a very large data pool. This creates four sets of probiotic recommendations, which you’ll need to manually review—look for overlaps in suggestions or options that none of the sets disagree with.
MP can also use identified nutrients to suggest which foods to include or avoid in the diet.
I am a statistician by training and experience. A common problem with people is to project causation on a random association (often of thousands possible) that agrees with ideological beliefs or doctrines. In this post, I will look at the dramatic increase of autism through the eyes of statistican. I will not be documenting the shyte out of things, just hitting highlights with many borrowed graphics.
The Reality
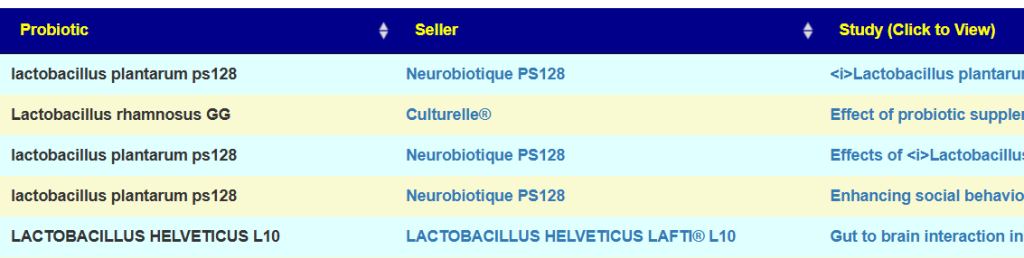
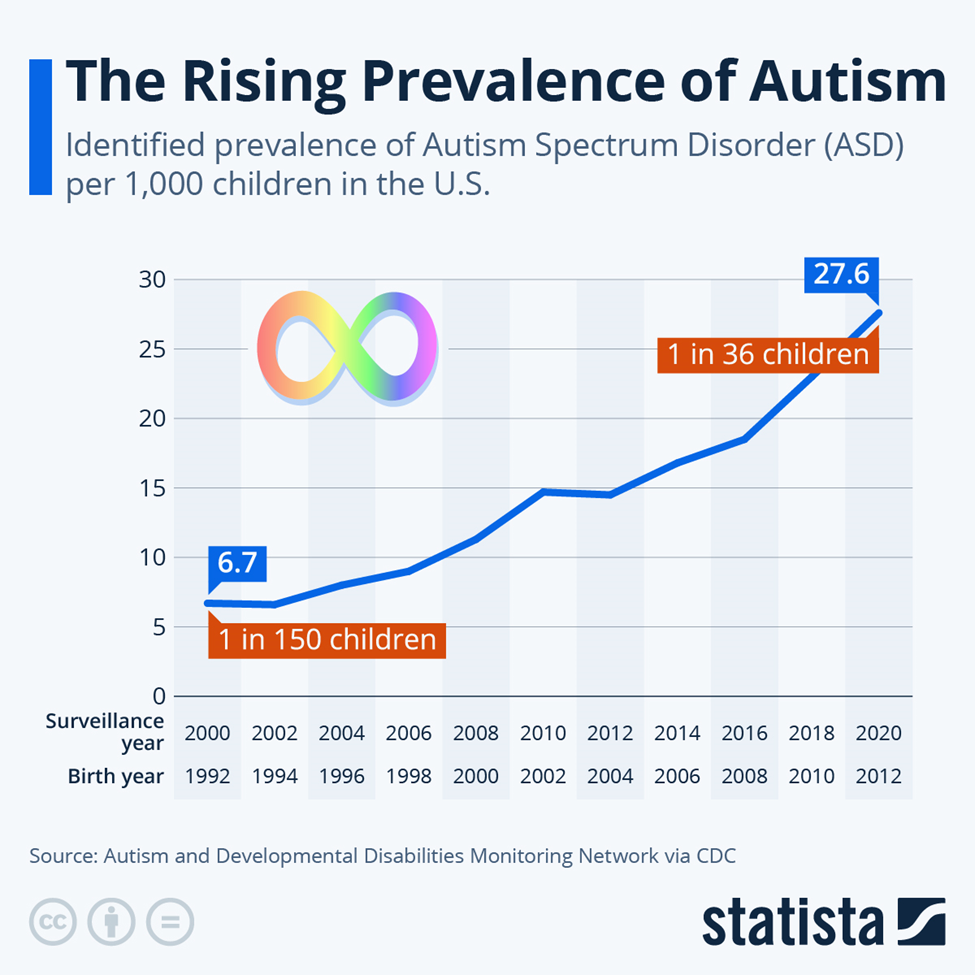
Before the 1960s, autism was considered a very rare condition, with prevalence estimates around 0.05% (1 in 2,000 children). This contrasts with recent estimates, which are significantly higher. Some studies from the 1960s and 70s reported prevalence rates between 2 and 4 cases per 10,000 children.
Vaccines
First, a 2025 study Large Danish Study: No link between vaccines and autism or 49 other health conditions using data from a national medical system (i.e. uniformity of treatment and records) with a high degree of uniformity in nutrition and other compounding analysis issues — effectively should end this red-herring that is popular in MAGA groups
Simple Culture Changes
A few years ago I wrote Autism Factors where I reviewed what was found to be very statistically significant including the following:
Age of mother
Caesarean delivery
Breast Feeding
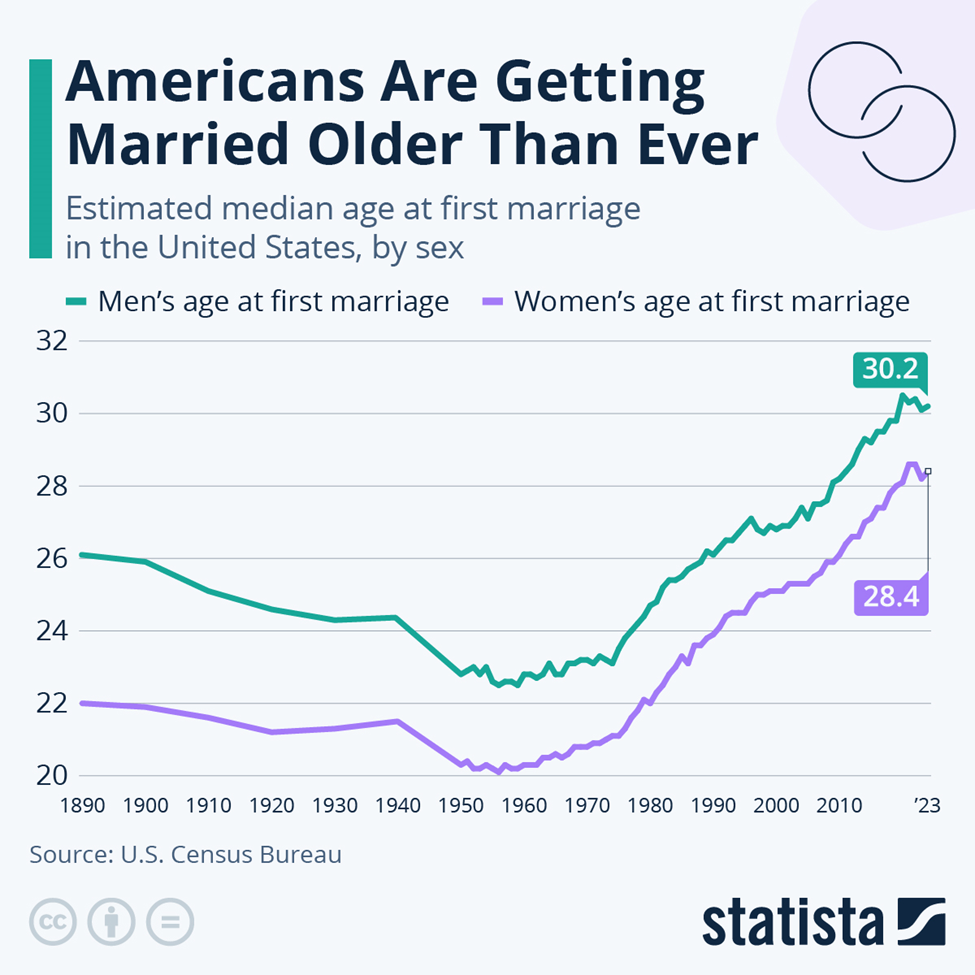
Marrying Older means more Autism
The increase of age shown below follow the above curve well!
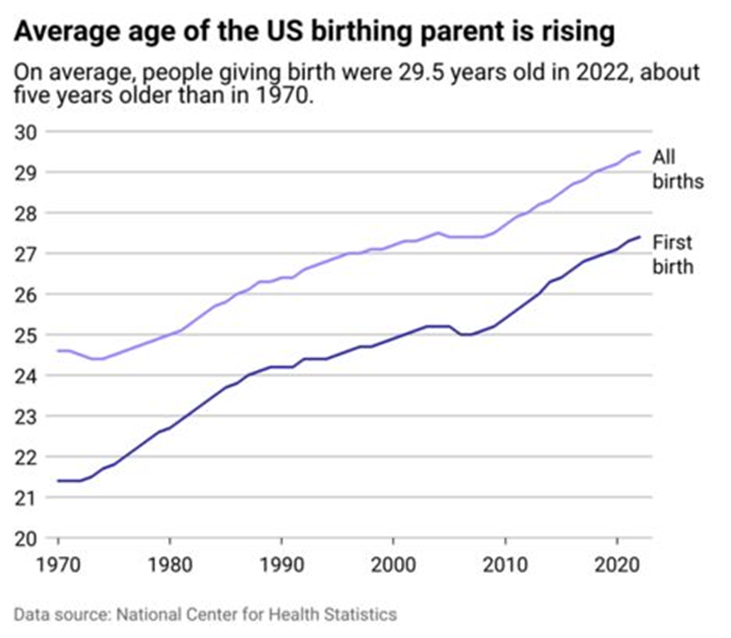
We also see that in age of birthing parents. Notice that both above and below, we have a flatening around 2010.
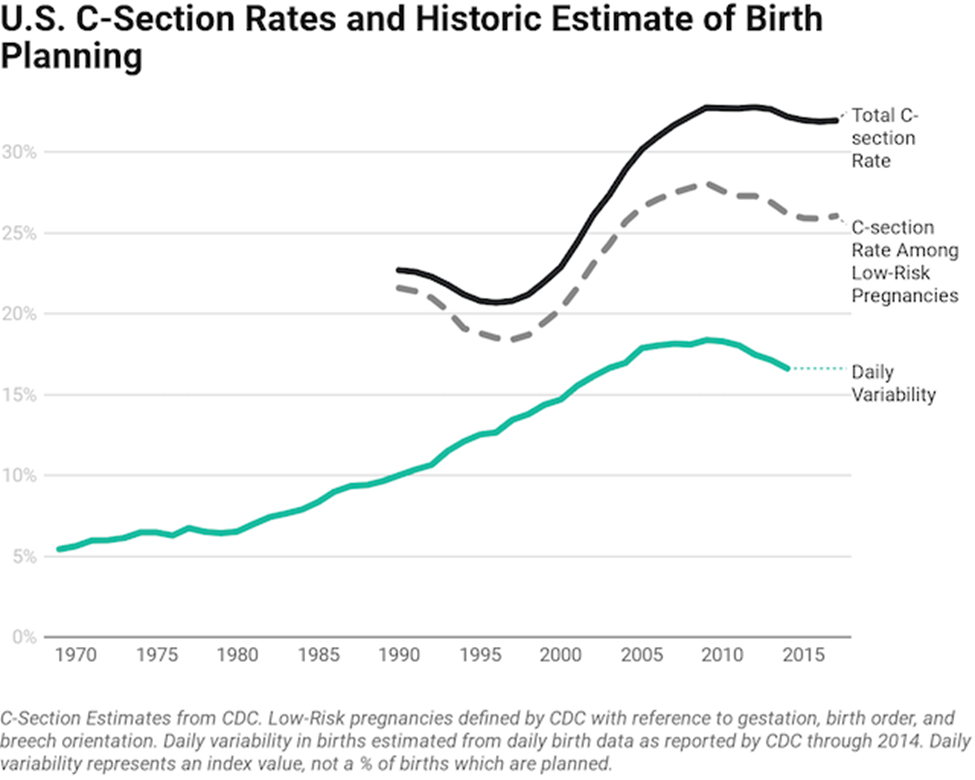
Looking at C-Sections, we seem more matching of patterns. Also breastfeeding decreases risk of autism.
Less Kids –> More Autism
Studies have revealed that the odds of a first child having autism is 160% of the chance of a second child. As the number of kids decrease, the number of kids with autism will increase. Assuming that everyone has one kid and 16/1000 has autism. With an average of 4 kids, it should drop to 11/1000. That is a 32% drop in the rate of autism
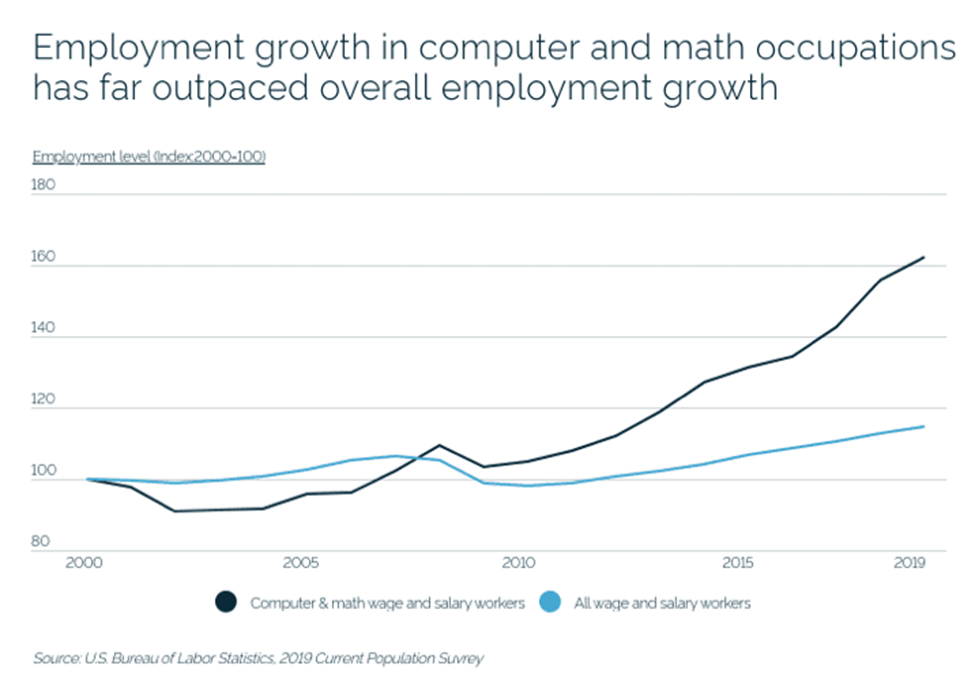
“Inbreeding”
Additional studies found increase incidence when both parents are involved with mathematics and computers. It has been suggested that DNA mutation that allows people to be successful in those occupations effectively increased the odd of an “in-breeding like” child. One mutation is fine, matching mutations is horrible.
Environmental Factors
The chart below makes this potential clear. “We found the previously reported relationship between precipitation and autism in a county was dependent on the amount of drinking water derived from surface sources in the county.” [2012]
The study, published Thursday in the Journal of Autism and Developmental Disorders, raises the possibility that parents in wealthier counties are successfully reducing environmental exposures that may contribute to autism risk, or taking other steps to curb its severity early on.
Autism is not purely genetic in a strict sense (if may be a significant factor), but age of birth, birth order, mother’s environmental issues are significant factors. All of these are “before the fact” issue. The best options for “after the fact” appear to be:
Environment
Microbiome manipulation
Concerning drugs, most drugs alter the microbiome and it is unclear if the drug is directly causing improvement, or indirectly by altering the microbiome.
The data that tend to follow or correlate alongside autism rate—meaning demographics, diagnostic trends, or related variables often tracked or reported with autism prevalence—include:
Age: Autism diagnoses are most commonly made in early childhood, especially between ages 2 and 8. Prevalence estimates are often reported for specific age cohorts, such as age 4 or 8, which the CDC uses for tracking trends.
Sex: A consistent male predominance is reported, usually about a 4-to-1 male-to-female ratio in childhood diagnoses. However, recognition of autism in girls lags behind, with many women diagnosed much later, suggesting under-identification in females.
Race/Ethnicity: Rates of diagnosis have historically been higher in white children, but recent data show increases among children of color as diagnostic access and awareness grow.
Socioeconomic Status: Diagnosis rates may connect to family income, healthcare access, and parental education, but increasing prevalence in different demographics may reflect better awareness and diagnostic efforts rather than true increases in incidence.
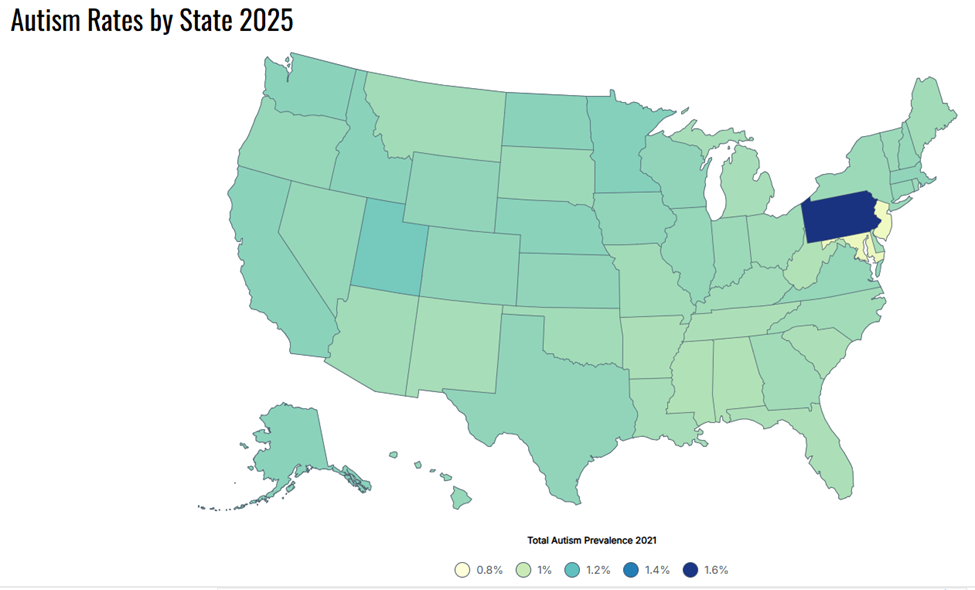
Geography: Autism prevalence varies by region and state, partly due to differences in healthcare systems, special education reporting, and diagnostic practices.
Method of Case Finding: Surveillance approaches (e.g., school/education records, medical billing data, or direct assessment) influence reported rates. Records-review surveillance and direct assessment generally yield higher prevalence than administrative counts.
Comorbid Conditions: Many studies note higher rates of intellectual disability, ADHD, anxiety, or other neurodevelopmental issues reported in those diagnosed with autism.
Time: Time trends are a key data point. Autism prevalence has risen substantially since the 2000s, largely attributed to broader diagnostic criteria, greater awareness, and increased screening—not necessarily a true rise in underlying incidence.
Diagnosis Age and Early Identification: Data often track the percentage of children diagnosed by a certain age, as early diagnosis is important for access to services.
Why not just use studies? There is nothing wrong with using studies. Pages listing studies result are linked to from each of the above pages. The difference is that with this approach you get the relative impact (R2) between probiotics which is not available from the studies. Also, some probiotics have very few studies, i.e. Lactococcus cremoris. Using both published studies and this tool gives the maximum coverage.
Recently I have been updating the statistic processing for association though diverse methods. Everything below is P < 0.005 (or 1 in 200 of happening at random).
From Ombre data
Bacteria
Rank
Shift
Bifidobacterium bifidum
species
Too High
Bifidobacterium subtile
species
Too High
Hungateiclostridiaceae
family
Too High
Liquorilactobacillus
genus
Too High
Liquorilactobacillus vini
species
Too High
Neisseriaceae
family
Too High
Peptoniphilus obesi
species
Too Low
Senegalimassilia
genus
Too High
unclassified Clostridiales
family
Too High
From Biomesight Data
One note, we do 4 different computations and in general they agree with each other (the Monte Carlo or Consensus Model). For Bifidobacterium species, that is not the case, some computations suggests too high and other computations suggests too low. Bifidobacterium with Autism have a variety of disagreements between studies. In this case, we know that the disagreement is due to the statistical method used.
As seen below, there is over prevalence (seen more often), but the values are smaller than the reference population.
Bacteria
Rank
Statistical Test
P Value
Shift
Bifidobacterium angulatum
species
Chi-2 prevalence
3.21E-12
Too High
Bifidobacterium angulatum
species
Mann_Whitney_Wilcoxon
0.000456655
Too Low
Bifidobacterium angulatum
species
Averages
0.000464826
Too Low
Bacteria
Rank
Shift
Absiella
genus
Too High
Acidaminococcus
genus
Too High
Actinomyces
genus
Too Low
Actinomycetaceae
family
Too Low
Actinomycetes
class
Too Low
Actinomycetota
phylum
Too Low
Agromyces
genus
Too High
Agromyces salentinus
species
Too High
Amoebophilaceae
family
Too High
Anaerotruncus
genus
Too High
Anaerotruncus colihominis
species
Too High
Anaerovibrio
genus
Too High
Anaerovibrio lipolyticus
species
Too High
Bacteroides
genus
Too High
Bacteroides cellulosilyticus
species
Too High
Bacteroides faecis
species
Too High
Bacteroides finegoldii
species
Too High
Bacteroides fragilis
species
Too Low
Bacteroides rodentium
species
Too High
Bacteroides stercorirosoris
species
Too High
Bacteroides thetaiotaomicron
species
Too High
Bacteroides uniformis
species
Too High
Bifidobacteriaceae
family
Too Low
Bifidobacteriales
order
Too Low
Bifidobacterium
genus
Too Low
Bifidobacterium adolescentis
species
Too Low
Bifidobacterium angulatum
species
Too High
Bifidobacterium angulatum
species
Too Low
Bifidobacterium bifidum
species
Too Low
Bifidobacterium catenulatum
species
Too High
Bifidobacterium catenulatum
species
Too Low
Bifidobacterium catenulatum PV20-2
strain
Too High
Bifidobacterium catenulatum PV20-2
strain
Too Low
Bifidobacterium catenulatum subsp. kashiwanohense
subspecies
Too High
Bifidobacterium catenulatum subsp. kashiwanohense
subspecies
Too Low
Bifidobacterium choerinum
species
Too Low
Bifidobacterium cuniculi
species
Too High
Bifidobacterium gallicum
species
Too High
Bifidobacterium gallicum
species
Too Low
Bifidobacterium indicum
species
Too High
Bifidobacterium indicum
species
Too Low
Bifidobacterium longum
species
Too Low
Bifidobacterium scardovii
species
Too High
Bifidobacterium subtile
species
Too Low
Burkholderia
genus
Too Low
Burkholderiales genera incertae sedis
no rank
Too Low
Caloramator fervidus
species
Too High
Caloramator indicus
species
Too High
Candidatus Amoebophilus
genus
Too High
Candidatus Amoebophilus asiaticus
species
Too High
Candidatus Blochmanniella
genus
Too High
Candidatus Blochmanniella camponoti
species
Too High
Clostridium
genus
Too High
Clostridium chartatabidum
species
Too High
Clostridium thermosuccinogenes
species
Too High
Collinsella aerofaciens
species
Too Low
Coriobacteriia
class
Too Low
Desulfotomaculaceae
family
Too High
Desulfovibrio
genus
Too High
Desulfuromonadaceae
family
Too Low
Desulfuromusa
genus
Too Low
Enterobacter
genus
Too Low
Enterobacter cloacae complex
species group
Too High
Enterobacter hormaechei
species
Too High
Enterobacterales
order
Too Low
Enterobacteriaceae
family
Too Low
Enterobacteriaceae incertae sedis
no rank
Too High
Erysipelothrix
genus
Too High
Escherichia
genus
Too Low
Escherichia coli
species
Too Low
Eukaryota
superkingdom
Too Low
Gammaproteobacteria
class
Too Low
Geopsychrobacteraceae
family
Too Low
Hathewaya
genus
Too High
Hathewaya histolytica
species
Too High
Hungateiclostridiaceae
family
Too High
Hungateiclostridium
genus
Too High
Hydrogenophilaceae
family
Too Low
Hydrogenophilales
order
Too Low
Hydrogenophilia
class
Too Low
Klebsiella oxytoca
species
Too High
Megamonas
genus
Too High
Megamonas
genus
Too Low
Megamonas funiformis
species
Too High
Megamonas funiformis
species
Too Low
Moorella group
norank
Too High
Oscillospira
genus
Too High
Parascardovia
genus
Too High
Parascardovia
genus
Too Low
Pedobacter
genus
Too High
Peptoniphilaceae
family
Too High
Peptoniphilus
genus
Too High
Phascolarctobacterium succinatutens
species
Too High
Phocaeicola
genus
Too High
Phocaeicola paurosaccharolyticus
species
Too High
Phocaeicola sartorii
species
Too High
Phocaeicola vulgatus
species
Too High
Porphyromonas
genus
Too High
Pseudoclostridium
genus
Too High
Rhodothermales
order
Too High
Rhodothermia
class
Too High
Rhodothermota
phylum
Too High
Sarcina
genus
Too Low
Sarcina maxima
species
Too Low
Segatella
genus
Too Low
Segatella albensis
species
Too Low
Segatella copri
species
Too Low
Segatella oulorum
species
Too High
Selenomonas
genus
Too High
Selenomonas infelix
species
Too High
Sphingobacteriaceae
family
Too High
Sphingobacteriales
order
Too High
Sphingobacteriia
class
Too High
Sphingobacterium bambusae
species
Too High
Streptococcus intermedius
species
Too High
Streptococcus mutans
species
Too High
Streptococcus thermophilus
species
Too Low
Thiomonas
genus
Too Low
Tissierellales
order
Too High
unclassified Bacteroidetes Order II.
order
Too High
Veillonella
genus
Too Low
Veillonella montpellierensis
species
Too Low
High Functioning Autism
We have smaller sample size, but do have some significant items
Statistics is fun because there many paths. Most studies using the microbiome uses the easy, but naïve, path of computing averages and standard deviation. As my dataset has grown, I have been travelling some less traveled path, for example: Visual Exploration of Odds Ratios, and a patent pending method termed “Kaltoft-Moltrup”.
One of the frequent decisions that I see in studies is to limit examination of bacteria that have a high frequency in the samples. This allows the researchers to keep to familiar and classic statistics. Using frequency of observation in the control group and the condition group is one of these much less travelled paths. It usually require big sample sizes and many studies have a sample size of 30 (sufficient for the mean and standard deviation approach).
I just completed code to compute Chi2 using Biomesight data for users reporting Autism.
Control Population: 3525
Autism: 88
Chi2 can be converted to probability (p) of happening at random with the following table
Seen too Rarely(Want to increase)
We see one bacteria available as a probiotic Bifidobacterium adolescentis. The rest would need to be altered by diet.
tax_name
TAX_RANK
Chi2
Observed
Expected
Shift
Butyricimonas synergistica
species
10
17
36
Under-Represented
Bifidobacterium adolescentis JCM 15918
strain
9.8
9
24
Under-Represented
Dehalobacterium
genus
9.7
18
37
Under-Represented
Pelotomaculum isophthalicicum
species
8
17
33
Under-Represented
Ammonifex thiophilus
species
7.3
17
32
Under-Represented
Seen too Often (Want to decrease)
We see 32 bacteria over a Chi2 of 6.635 ( P < 0.01 or 1 change in 100 of being a false detection). One very striking feature is that there are many, many different species of Bifidobacterium that are over represented while one species is under represented. This is not a simple situation to address.
tax_name
TAX_RANK
Chi2
Observed
Expected
Shift
Bifidobacterium catenulatum subsp. kashiwanohense
subspecies
43.5
54
23
Over-Represented
Bifidobacterium angulatum
species
33
39
16
Over-Represented
Staphylococcus pseudolugdunensis
species
23.6
20
7
Over-Represented
Clostridium cellulovorans
species
22.9
20
7
Over-Represented
Bifidobacterium catenulatum PV20-2
strain
19.5
58
33
Over-Represented
Streptococcus mutans
species
19
23
10
Over-Represented
Hungateiclostridium
genus
18.3
30
14
Over-Represented
Hungateiclostridiaceae
family
18.1
30
14
Over-Represented
Streptococcus intermedius
species
17.5
23
10
Over-Represented
Bifidobacterium catenulatum
species
16.9
58
34
Over-Represented
Absiella
genus
16.7
22
10
Over-Represented
Clostridium chartatabidum
species
16.7
43
23
Over-Represented
Bifidobacterium gallicum
species
15.4
73
47
Over-Represented
Prevotella veroralis
species
13
15
6
Over-Represented
Corynebacterium durum
species
12.6
14
6
Over-Represented
Bifidobacterium thermacidophilum
species
11.3
18
8
Over-Represented
Parascardovia
genus
10.5
32
18
Over-Represented
Klebsiella oxytoca
species
10.5
27
15
Over-Represented
Bifidobacterium scardovii
species
10
30
17
Over-Represented
Bifidobacterium cuniculi
species
9.9
31
18
Over-Represented
Candidatus Blochmanniella camponoti
species
9.8
21
11
Over-Represented
Abiotrophia
genus
9.2
12
5
Over-Represented
Enterococcus gilvus
species
9.1
14
6
Over-Represented
Megamonas funiformis
species
8.8
21
11
Over-Represented
Segatella oulorum
species
8.6
22
12
Over-Represented
Ralstonia
genus
7.9
14
7
Over-Represented
Bifidobacterium indicum
species
7.7
67
48
Over-Represented
Candidatus Blochmanniella
genus
7.2
35
22
Over-Represented
ant endosymbionts
clade
7.2
35
22
Over-Represented
unclassified Bacteroidetes Order II.
order
7.2
75
55
Over-Represented
Enterobacter hormaechei
species
6.9
36
23
Over-Represented
Moorella group
norank
6.7
66
48
Over-Represented
Bottom Line
The next step is to compute similar tables for all symptoms and incorporate these findings into a new algorithm. I say new, because I do not know if it is better than the existing ones. Conceptually, it would be added as a 5th set of suggestions to the existing consensus view on Microbiome Prescription.
This is a preview of the next generation of analysis. I described a mathematical model in Microbiome Guilds, Metabolites and Enzymes. I mentioned a concept in it and over the weekend tried the concept out. It worked and is very sweet.
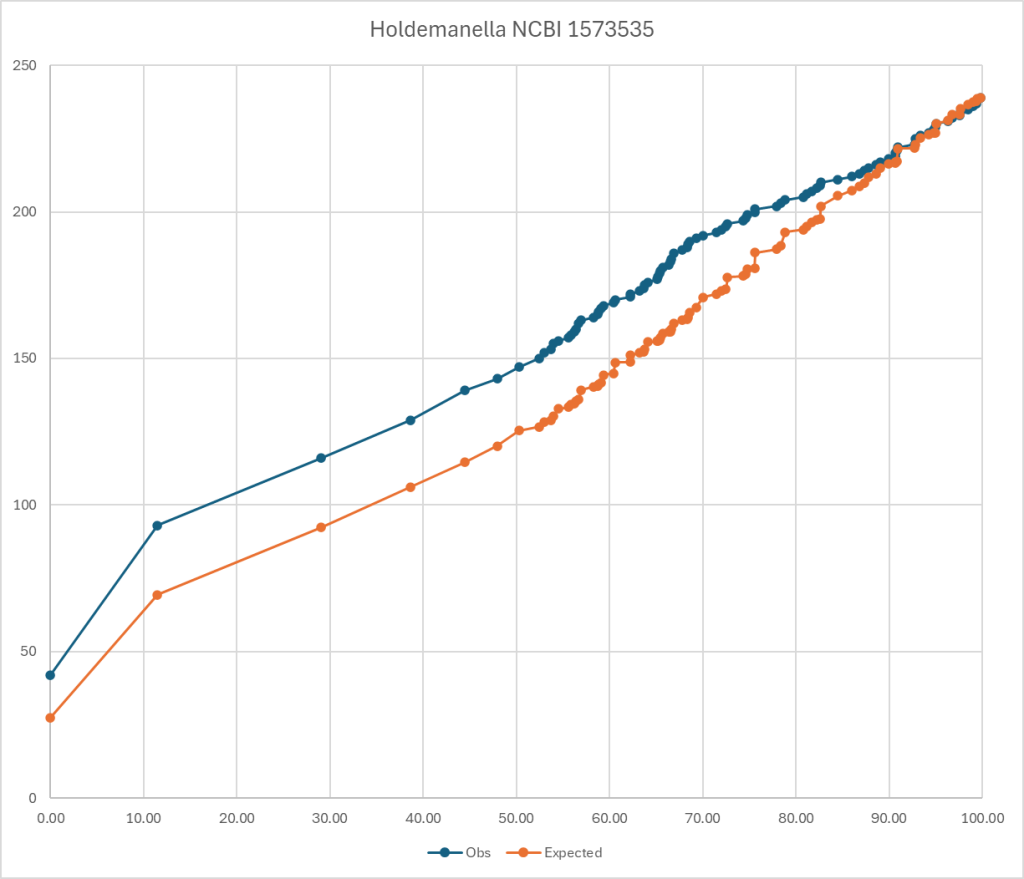
To explain it, look at the chart below. The blue line is for those that have a symptom and the orange line is what is expected. If you divide observed by expected for different percentiles, you get an odds ratio. Most people know odds ratio (OR) from things like:
For current male smokers consuming >30 cigarettes daily:
This pattern does not determine that you will absolutely get it. It means that your are more likely — odds. (My native environment as a statistican)
This means that we move from a vague hand-waving “Too high” or “Too Low” to actual numbers (percentiles to be precise, not percentages).
Biomesight Bacteria
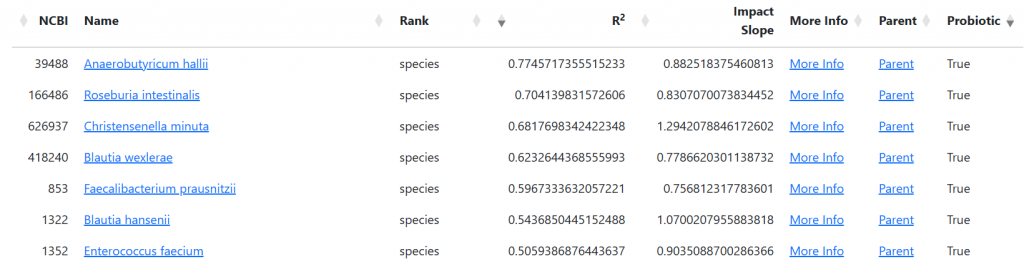
The genus bacteria listed below, each have at least an odds ratio of 1.5 for general fatigue using Biomesight data if your percentile is below the amount show. I stopped listing at 10%ile items. Compared to my earlier post for Bacteria Associated with General Fatigue, we have some really string candidates – 90!. 96 means 96%ile.
If you have 10 of them then 1.5 ^ 10 = 57x greater odds of having general fatigue. It is NOT one bacteria causing it, or even a specific group of bacteria, but different combinations of possible bacteria.
I should mention that these numbers only applies to Biomesight data. “results from one pipeline cannot be safely applied to another“. For background see: The taxonomy nightmare before Christmas.
. It potentially allows a screening test to be done for autism from a microbiome sample (and also hints at what specifically needs to be corrected).
Chlorobaculum >= 96
Roseococcus >= 94.9
Marichromatium >= 93.8
Ectothiorhodospira >= 93.8
Aquimonas >= 93.5
Xenophilus >= 92.5
Neorickettsia >= 90.9
Syntrophobacter >= 90
Pelomonas >= 88.5
Trichococcus >= 88
Steroidobacter >= 86.5
Desulfofrigus >= 65
Hathewaya <= 47.6
Pseudoclostridium <= 42.2
Desulfovibrio <= 37.9
Anaerovibrio <= 37.1
Ehrlichia <= 36.1
Phocaeicola <= 36
Johnsonella <= 30
Acetobacterium <= 27.6
Candidatus Amoebophilus <= 27.2
Oscillospira <= 25.2
Anaerotruncus <= 25.1
Erysipelothrix <= 24.9
Bacteroides <= 24.6
Porphyromonas <= 21.2
Selenomonas <= 21
Pedobacter <= 20.1
Ombre Equivalent Bacteria
If you have Ombre’s microbiome results, these are the critical bacteria. It is a much smaller list then above (and as expected, very few bacteria names in common — “the nightmare”)
Cystobacter >= 95.8
Cellulomonas >= 95.2
Tannerella <= 39.6
Erysipelatoclostridium <= 34.7
Alistipes <= 29.1
Alloprevotella <= 28.8
Phocaeicola <= 28.6
Oleidesulfovibrio <= 27.6
Pseudoflavonifractor <= 27.5
Odoribacter <= 25.6
Ethanoligenens <= 24.9
Pedobacter <= 24.3
Leyella <= 23.8
uBiome Equivalent Bacteria
There was not sufficient data to compute bacteria odds ration
Metabolites
I did a follow up post using Odds Ratio with Metabolites in the context of ME/CFS.
Metabolite-Centric Analysis
Bacterial Metabolic Activity: Bacteria produce and consume various metabolites, which can significantly impact the host’s metabolic environment13.Metabolic Imbalances: Different bacterial compositions can lead to similar metabolite imbalances, making metabolite profiles potentially more informative than bacterial species profiles alone7 8.
Advantages of This Approach
Net Effect: By examining metabolites, we can assess the overall impact of the microbiome on the host, regardless of the specific bacterial species present5.
Consistency: Metabolite imbalances may be more consistent across patients than bacterial species composition, which can vary widely7.
Functional Insight: This approach provides insight into the functional consequences of microbiome dysbiosis in ME/CFS3 8.
Understanding metabolite profiles in ME/CFS could lead to:
Improved diagnostic tools
Identification of potential therapeutic targets
Personalized treatment approaches based on individual metabolic profiles58
I am showing the numbers for Biomesight sample below. Conclusions across Ombre, uBiome and Biomesight are at the bottom.
Warning: These are the chemical names — a few are available as supplements with more common name.
Looking for Metabolites shared between Ombre and Biomesight samples, only a single metabolite was flagged by both for low: Hydroquinone (1.6%ile for Ombre, 26%ile for Biomesight).
Ombre flagged some 510 metabolites, while Biomesight flagged 542 metabolites. Too much to drill down into. So let us look at the shared one above in more detail.
Based on the Perplexity search results, hydroquinone has shown some interesting connections to cognitive functions, particularly in the context of brain injury and neuroprotection:
Neuroprotective Effects
Hydroquinone (HQ) has demonstrated significant neuroprotective properties in experimental models of brain injury:
In a rat model of transient focal cerebral ischemia, HQ treatment strongly alleviated ischemic brain injury3 4.
The neuroprotective effect of HQ was associated with the prevention of blood-brain barrier (BBB) disruption3. This is crucial because the BBB plays a vital role in maintaining brain homeostasis and protecting cognitive functions.
HQ treatment maintained the expression of tight junction proteins in the ischemic cortex, which are essential for BBB integrity3.
Potential Cognitive Benefits
While not directly tested for cognitive enhancement, the neuroprotective effects of HQ suggest potential cognitive benefits:
By preventing BBB disruption, HQ may help maintain normal brain function and protect against cognitive decline associated with ischemic events3.
Both pre- and post-treatment with HQ showed protective effects against ischemic damage in experimental models6. This suggests potential applications in both preventive and therapeutic contexts for cognitive protection.
Considerations and Limitations
It’s important to note some limitations and considerations:
Most studies on HQ’s neuroprotective effects have been conducted in animal models, and more research is needed to confirm these effects in humans3 4.
The typical use of HQ as a skin-lightening agent is unrelated to its potential cognitive effects5. Its primary application remains in dermatology.
High doses or long-term use of HQ may have adverse effects. A study on percutaneous drug delivery showed that high doses of HQ could impair hippocampal structure and induce behavioral disorders in mice1.
In conclusion, while hydroquinone shows promising neuroprotective effects that could potentially benefit cognitive functions, especially in the context of brain injury, more research is needed to fully understand its impact on human cognition and to determine safe and effective applications beyond its current use in dermatology.
Bottom Line
Adding this to the website to allow individual analysis of individual microbiome is high on my backlog. One of the benefits is the ability to focus on specific bacteria being at specific levels which conceptually should result in better suggestions.
Since it is deficiency, we look for an alternative supply from bacteria in the microbiome. There are many bacteria that has the capacity of producing it, but the enzyme may not be turned on (epigenetics). I was directed by perplexity to Wikipedia. This identifies a bacteria that is likely a high (actual) producer.
Leuconostoc mesenteroides: This bacterium has been shown to possess a G6PD enzyme that is reactive toward 4-hydroxynonenal, in addition to glucose-6-phosphate
This bacteria is available as a probiotic (one source).
General Information about Autism Enzymes and Compound Production
From the hundreds of donated microbiome samples annotated with Autism on Microbiome Prescription, I have done some statistical analysis (using a patent pending method for partitioning samples), “poor man metagenomics”, and have produce a summary on those who have an official diagnosis of autism.
First, I checked if EC 1.1.1.49 was on the list. It was not, which implies that is not a very common item across all autism patients.
Browsing the lists I did find two familiar items being high:
(R)-Lactate – also known as d-lactic acid, a common cause of brain fog and other neurological conditions see this for a list.
L-Histidine which is likely a protective feature (more information)
The amount of (R)-Lactate reported above was computed from the microbiome data which implies that reducing its level by microbiome manipulation is a viable path.
Modelling on an individual sample
With recent revisions of the UI, I have built an algorithm to select the probiotics that supply the maximum amount of these KEGG compounds and Enzymes that most meet the deficiencies detected.
To illustrate this feature, I took one of the autism samples upload and ask for the suggestions.
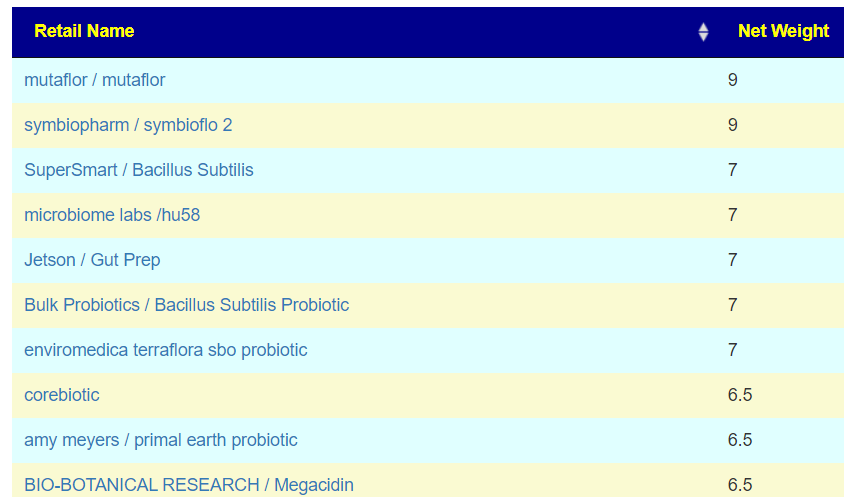
Below is the results of probiotics to increase the low KEGG compound in this sample.
Below is the results of probiotics to increase the low KEGG Enzymes in this sample. They are reasonably close to each other.
Bottom Line
This is all theoretical, but as probiotics are usually deemed to be safe and without significant risks, it is a possible experiment to try. Always take detail notes and report benefits and problems as comments on this post
It is interesting to note that the common Lactobacillus and Bifidobacterium are not need the top of either list.
An older video on the process
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
My preferred provider for herbs etc is Maple Life Science™ – they are all organic, fresh, without fillers, and very reasonably priced.
Professional Medical Review Recommended
Individual health conditions may make some suggestions inappropriate. Mind Mood Microbes outlines some of what her consultation service considers: A comprehensive medical assessment should consider:
Terrain-related data
Signs of low stomach acid, pancreatic function, bile production, etc.
Detailed health history
Specific symptom characteristics (e.g., type and location of bloating)
I am doing a normalization and update of data on Microbiome Prescription. There are many items to review and items that have been reviewed have { } in their name. The pattern is:
Scientific Name
{Common Name}
Other Information
and not reviewed (YET)
So far in this review, I have come across two substances (more likely to come) where there has been many or interesting studies for Autism
Sulforaphane
This is found in broccoli sprouts,cauliflower, kale, cole crops, cabbage, collards, mustard, and cress
“Furthermore, it has been reported that most infant formulas are contaminated with glyphosate. One study reported levels between 0.03 mg kg−1 and 1.08 mg kg−1. This could potentially further exacerbate the problem of Bifidobacterium reduction in the infant gut.” This may be a factor for increasing Autism and ADHD rates.





Recent Comments